|
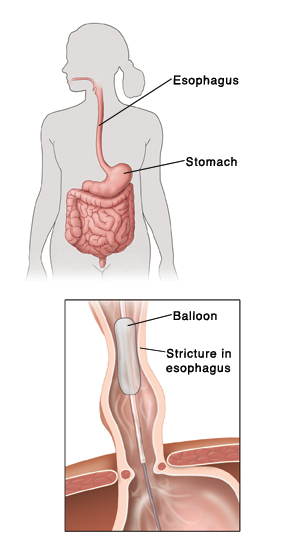
What is Achalasia Treatment Achalasia is a phenomenal gulping issue that influences around 1 in every 100,000 individuals. The significant side effect of Achalasia Cardia is normally trouble with gulping. The vast majority are diagnosed between the ages of 25 and 60 years. In spite of the fact that the condition can't be cured, the indications can more often than not be controlled with treatment. Achalasia Causes In achalasia, nerve cells in the throat (the tube that conveys nourishment from the mouth to the stomach) ruffian for reasons that are not known. The loss of nerve cells in the throat causes two noteworthy issues that meddle with gulping: The muscles that line the throat don't contract typically, so that gulped sustenance is not impelled through the throat and into the stomach appropriately. The lower esophageal sphincter (LES), a band of muscle that circles the lower segment of the throat, does not work effectively. Ordinarily, the LES unwinds when we swallow to permit gulped sustenance to enter the stomach. At the point when the sustenance has traveled through the throat into the stomach, the LES muscle contracts to crush the end of the throat shut, accordingly keeping the stomach substance from streaming in reverse (refluxing) into the throat. In individuals with achalasia, the LES neglects to unwind typically with gulping. Rather, the LES muscle keeps on pressing the end of the throat, making an obstruction that keeps sustenance and fluids from going into the stomach. Over the long run, the throat over the constantly contracted LES widens, and extensive volumes of nourishment and spit can collect in the expanded throat. Achalasia Symptoms The most well-known side effect of Achalasia Symptoms is trouble gulping. Patients frequently encounter the vibe that gulped material, both solids and fluids, gets stuck in the midsection. This issue regularly starts gradually and advances progressively. Numerous individuals don't look for help until indications are progressed. A few individuals repay by eating all the more gradually and by utilizing moves, for example, lifting the neck or tossing the shoulders back, to enhance discharging of the throat. Different manifestations can incorporate midsection torment, disgorging of gulped nourishment and fluid, acid reflux, trouble burping, a vibe of totality or a protuberance in the throat, hiccups, and weight reduction. Achalasia Diagnosis Achalasia may be suspected based upon manifestations, however tests are expected to affirm the analysis. Midsection x-beams — A midsection x-beam may uncover an enlarged throat and nonattendance of air in the stomach. In any case, a midsection x-beam is not sufficient for a finding of What is Achalasia and further testing is needed. Barium swallow test — The barium swallow test is a typical screening test for achalasia. The test includes gulping a pasty tasting, thick mixture of barium while x-beams are taken. The barium demonstrates the framework of the throat and lower esophageal sphincter (LES). Trademark discoveries of achalasia on barium swallow incorporate a tirelessly contracted area toward the end of the throat (the LES), with a widened throat over the limited district. The barium swallow might likewise indicate spastic compressions in the throat over the LES, a condition called "incredible achalasia". Esophageal manometry (additionally called esophageal motility study) — Manometry is a test that measures changes in weights inside the throat that are created by the constriction of the muscles that line the throat. The test includes the section of a dainty tube through the mouth or nose into the throat. The tube is lined by various weight sensors that pass on weights inside the throat to a gadget that records those weights. Patients are typically taught to have nothing to eat or beverage for eight hours prior to the test, and they are given tastes of water to swallow while the tube is set up. Manometry is quite often used to affirm the determination of achalasia. The test normally uncovers three variations from the norm in individuals with achalasia: high weight in the LES very still, disappointment of the LES to unwind in the wake of gulping, and a nonattendance of helpful (peristaltic) compressions in the lower throat. The last two highlights are the most critical and are obliged to make the conclusion of achalasia. Endoscopy — Endoscopy permits the doctor to see within the throat, LES, and stomach utilizing a slender, lit, adaptable tube. Most patients are given narcotics amid the endoscopy technique. This test is typically suggested for individuals with suspected achalasia and is particularly helpful for distinguishing different conditions that can impersonate achalasia, for example, disease of the upper part of the stomach. In individuals with achalasia, endoscopy frequently uncovers a widened throat that contains held nourishment; it might likewise uncover aggravation, little ulcers brought on by leftover sustenance or pills, and candida (yeast) disease. The endoscope can be progressed through the LES and into the stomach to check for stomach malignancy. Malignancy in the upper piece of the stomach can create indications and irregular manometry results that are essentially indistinguishable to those of achalasia. This condition is called pseudoachalasia (signifying "false" achalasia) or optional achalasia. Biopsies (little examples of tissue) are frequently gotten in the lower part of the throat to search for malignancy cells. Having a biopsy of the throat taken amid endoscopy is not difficult and is by and large a safe strategy. Achalasia Treatment A few choices are accessible for the Achalasia Treatment. Sadly, none can stop or opposite the hidden loss of nerve cells in the throat of patients with achalasia. Notwithstanding, the medicines are typically compelling for enhancing side effects. None of the accessible medications are required to restore typical (peristaltic) withdrawals in the throat of patients with achalasia. Maybe, the medicines mean to debilitate the lower esophageal sphincter (LES) muscle to the point that it no more represents an obstruction to the entry of sustenance. The LES can be debilitated by medications, or mechanically by strategies that tear or cut the LES muscle. Drug treatment — Two classes of medications, nitrates and calcium channel blockers, have LES muscle-unwinding impacts. These medications can diminish manifestations in individuals with achalasia. The medications are normally taken by putting a pill under the tongue 10 to 30 minutes prior to dinners. Drug treatment is the minimum intrusive and most secure alternative for treating achalasia. In any case, a great many people find that long haul drug treatment is awkward, ineffectual, and regularly connected with upsetting symptoms, for example, cerebral pain and low pulse. Moreover, the medications have a tendency to end up less compelling over the long run. Hence, prescriptions are prescribed basically for patients who are not inspired by or not sufficiently beneficial for mechanical medicines, for example, inflatable enlargement and surgery (myotomy). Inflatable enlargement (pneumatic dilatation) — For blow up expansion, the patient swallows a crumpled blow up that is situated in the LES. A x-beam machine is frequently used to guide situation of the blow up. At the point when the inflatable has been situated at the LES, it is swelled unexpectedly to an expansive size with a specific end goal to tear the muscle of the LES. This system is viable for soothing the gulping trouble in patients with achalasia in more or less 66% of individuals, albeit midsection agony continues in some. Patients as often as possible require more than one blow up enlargement treatment for satisfactory help. Strategy — If you have inflatable expansion, you will be approached to drink fluids for 12 hours to two days ahead of time (a more extended period is prescribed on the off chance that you have a lot of sustenance maintenance in the throat). Utilizing endoscopy and fluoroscopy (x-beam), a doctor propels an aide wire down the throat and positions it inside the LES. A flattened blow up is then best in class along this aide wire, situated inside the LES, and expanded for a variable period extending from seconds to minutes. The inflatable is then flattened and withdrawn, and you are observed in a recuperation region for various hours to distinguish any muddlings. After the inflatable enlargement, a few doctors routinely perform a x-beam test like the barium swallow depicted above to verify that the blow up has not made a gap (aperture) in the throat. In the event that there are no complexities, you can generally resume eating when you have recuperated from the system. In the event that your regular manifestations don't enhance, extra enlargements can be performed. Achievement rate — A solitary inflatable enlargement session keeps on easing side effects of achalasia in around 60 percent of individuals one year after the system and in around 25 percent of individuals five years after the technique. Higher achievement rates have been accounted for in a few studies. The achievement rate after more periods has not been very much contemplated, but rather a few individuals have remained indication free the length of 25 years. Inconveniences — About 15 percent of individuals experience serious midsection torment instantly after blow up expansion and some experience fever. The most genuine difficulty of blow up widening is making of a gap (aperture) in the mass of the throat; this muddling happens in around 2 to 5 percent of individuals experiencing the strategy. Side effects of tireless or exacerbating agony in the hours after the technique may
0 Comments
|
AuthorJenifer Lawrance Archives
September 2016
Categories
All
|
 RSS Feed
RSS Feed
